6
English
Description
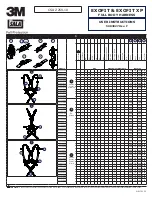
Pulsar-18 T3 Stent System (hereinafter Pulsar-18 T3) as shown in
Figure 1 is a self-expanding stent that is pre-mounted on an over-the-
wire delivery system.
The stent (1) is a permanent implant and made from a laser-cut
nitinol tube. The stent (1) has six radiopaque markers on either ends
(1a, 1b) and is completely covered with a thin layer of amorphous
silicon carbide (proBIO™).
The delivery system consists of a triaxial
shaft design: the inner shaft
assembly (2), the middle retractable shaft (3) and the fixed outer blue
stabilizer shaft (11).
The central guide wire lumen within the inner shaft assembly (2)
begins at the distal delivery system’s
tip (7) and ends at the luer port
(6) on the handle (9). The guide wire lumen is flushed through the
luer port (6).
The stent is positioned in-between the inner shaft assembly (2) and
the retractable shaft (3) on the distal end of the delivery system. The
two radiopaque markers on the delivery system (8a, 8b) facilitate
fluoroscopic visualization and the positioning of the stent system
towards and across the lesion.
The retractable shaft (3) begins within the handle (9) and extends
towards the delivery system’s tip (7). The retractable shaft (3) covers
the stent (1), keeping it constrained on the delivery system. The
moving radiopaque marker (10) on the retractable shaft (3) enables
visual control during stent deployment. The outer surface of the tip
(7), retractable shaft (3) and the blue stabilizer shaft (11) are covered
with a hydrophobic coating, and an anti-friction agent is applied
in-between the retractable shaft (3) and the inner shaft assembly (2).
The blue stabilizer shaft (11) is designed to reduce friction between
the stent system and the hemostatic valve of the introducer sheath.
The safety button in an unlocked position (4) and the rotating wheel (5)
on the handle (9) are used for stent (1) deployment.
How Supplied
Sterile. Non-pyrogenic. Device is sterilized with ethylene oxide.
Contents
• One (1) Stent system in a sealed, peel-open pouch.
• One (1) Instructions For Use manual and one (1) Patient Implant
Card.
Storage
Store protected from sunlight and keep dry. Store between 15°C and
25°C. Short-term storage temperature excursions between 10°C and
40°C are allowed.
Indications
Pulsar-18 T3 is indicated for use in patients with atherosclerotic
disease of the superficial femoral, proximal popliteal
and infra-
popliteal arteries and for the treatment of insufficient results after
percutaneous transluminal angioplasty (PTA), e.g. residual stenosis
and dissection.
Contraindications
Pulsar-18 T3 is contraindicated for use in patients with/who:
• Lesions judged to prevent proper treatment with the stent system,
including proper placement of the stent or complete inflation of an
appropriately-sized angioplasty balloon.
• Large amounts of acute or sub-acute thrombus at the target lesion.
• Perforated vessel.
• Lesion that lie within or adjacent to an aneurysm.
• Threatened occlusion of vital side branches.
• Uncorrected bleeding disorders or those who cannot receive the
recommended antiplatelet and/or anticoagulation therapy.
• Renal insufficiency or an allergy to contrast media.
• A known hypersensitivity to nickel or amorphous silicon carbide.
Warnings
• This device carries an associated risk of subacute thrombosis,
vascular complications and bleeding events. Therefore, careful
selection of patients is crucial. Antiplatelet therapy is advised for a
period of six months post-procedure.
• This device is designed and intended for single use only. DO NOT
resterilize and/or reuse. Reuse of single-use devices creates a
potential risk of patient or user infections. Contamination of the
device may lead to injury, illness or death of the patient. Cleaning,
disinfection and sterilization may compromise essential material
and design characteristics leading to device failure. BIOTRONIK
will not be responsible for any direct, incidental or consequential
damages resulting from resterilization or reuse.
• DO NOT use the stent system if the outer package and/or inner
package are/is damaged or opened, or if any information provided
is obscured or damaged. DO NOT use if the device is damaged or if
the stent is partially deployed.
• DO NOT use the device after the Use by date indicated on the label.
• DO NOT expose the stent system to organic solvents, e.g. alcohol.
• Manipulate the stent system under angiographic guidance when it
is in the patient’s body.
• If a large amount of thrombus is present in the vessel, the use
of alternative or adjunctive strategies (mechanical debulking,
thrombolysis, GPIIb/IIIa inhibitors) must be considered.
Precautions
General Precautions
• This device should only be used by physicians thoroughly trained
and experienced in performing vascular interventions, (including
cases of life-threatening complications).
• Fractures of nitinol stents implanted in the superficial femoral
artery have been reported in medical literature. Fractures occurred
more frequently and were more severe in long stented segments
and in the case of multiple, partially overlapping stents. These
fractures were frequently associated with restenosis or occlusion
of the artery.
• Precautions to prevent or reduce clotting should be taken. The use
of systemic heparinisation during the procedure is recommended.
Handling Precautions
• Prior to the procedure, the stent system should be visually
examined to verify functionality and ensure that its size is suitable
for the specific procedure for which it is to be used.
• Exercise care during handling to reduce the possibility of deploying
the stent prematurely, accidental breakage, bending or kinking of
the delivery system shaft.
Stent Placement Precautions
• Use only guide wires with a 0.018” (0.46 mm) diameter.
• Use only with an appropriately-sized introducer sheath indicated on
the label. If Pulsar-18 T3 is used in conjunction with long and/or
braided introducer sheaths, a larger French size than indicated on
the label may be necessary to reduce friction.
• DO NOT advance a partially deployed stent proximally or distally as
dragging of repositioning it may cause injury to the patient.
• DO NOT insert and advance the stent system in the body if the stent
system has not been threaded over a guide wire and the guide wire
does not extend beyond the delivery system’s tip to avoid vessel
damage.
• If strong resistance is felt during stent deployment, stop the
procedure and determine the cause before proceeding. If the stent
cannot be deployed, remove the entire stent system.
• The stent system is not designed for use with power injection
systems.
• If multiple stents are required to treat a lesion:
- Stents should be of similar composition as the risk of corrosion
increases when stents of differing metals contact one another.
- Overlapping of more than two stents have not been investigated.
- It is recommended to place the distal stent first and allow for
sufficient overlap between the stents.
• Recrossing a stent with adjunct devices must be performed with
caution.
• The use of mechanical atherectomy devices or laser catheter is not
recommended within the stented area.
• Stenting across a bifurcation may compromise future diagnostic or
therapeutic procedures.
Potential Adverse Events/Complications
Possible complications include, but are not limited to:
• Emergency surgery to correct vascular complications.
• Infection and sepsis.
• Allergic reactions to contrast media, antiplatelets, anticoagulants
and amorphous silicon carbide.
• Embolization of air, thrombotic or atherosclerotic material.
• Tissue necrosis and limb loss due to distal embolization.
• Stent system events: failure to deliver stent to intended site,
stent misplacement, stent deformation, stent embolization, stent
thrombosis or occlusion, stent fracture, stent migration, inadequate
apposition or compression of stent/s, withdrawal difficulties,
emboli zation of the delivery system material.
• Vascular events: access site hematoma, hypotension/ hypertension,
pseudoaneurysm, arteriovenous fistula formation, retroperitoneal
hematoma, vessel dissection or perforation, restenosis, thrombosis
or occlusion, vasospasm, peripheral ischemia, dissection and distal
embolization (air, tissue debris and thrombus).
• Bleeding events: access site bleeding or hemorrhage and hemor-
rhage requiring transfusion or other treatment.
• Death.
Directions for Use
Patient Preparation and Stent System
Selection
1. Prepare the patient and lesion site according to standard clinical
practice. Pre-dilation of the lesion using standard PTA techniques
before stenting is recommended.
2. Select an appropriate stent size based on the diameter of the
artery adjacent to the lesion and the length of the segment to
be stented according to the “Vessel Sizing” table on page 5. The
length of the stent should overlap the lesion by at least 5 mm on
either sides.
Stent System Preparation
3. Check and ensure that the outer packaging is not damaged or
opened prior to use. Open the outer packaging and remove the
pouch. Inspect the pouch and ensure that there is no damage to
the sterile barrier before proceeding. Open the pouch and remove
the sterile content.
4. Pick up the handle first from the tray then pull the delivery system
out from the protection ring and place it on the sterile field. Take
care not to kink the catheter. Examine the stent system for any
damage prior to use.
Flushing of the Guide Wire Lumen
5. Attach a 10 ml syringe filled with sterile heparinized saline to the
luer port at the proximal guide wire exit and inject at least 5 ml
saline into the guide wire lumen until the fluid exits the delivery
system’s tip as shown in Figure 2.
6. Remove the syringe.
Introduction of the Stent System
7. Examine the stent system for damage. Check to see that the distal
stent end is contained within the retractable shaft. DO NOT use the
stent system if the stent is exposed.
8. Thread the distal tip of the stent system over the proximal end
of the guide wire and advance until the guide wire exits the luer
port at the proximal end of the handle. Keep the stent system as
straight as possible.
9. Insert the stent system carefully through the introducer sheath
whilst immobilizing the guide wire. Verify that the distal end of the
retractable shaft is flush against the delivery system’s tip.
10. Carefully advance the stent system over the guide wire just distal
to the lesion to be treated.
11. Advance the stent system across the lesion and position the
markers on either sides of the lesion. Check that the blue
stabilizer shaft is inside the hemostatic valve. If the blue stabilizer
shaft cannot be kept inside, keep the delivery system as straight as
possible outside the patient’s body.
Stent Deployment
12. Maintain the stent system and guide wire as straight as possible
outside the patient’s body as shown in Figure 3. Any slack in the
delivery system may result in incorrect stent placement, potential
stent compression or elongation.
13. Press the safety button as shown in A of Figure 4 until it stays
locked in the pressed position.
14. Ensure that the positions of the distal and proximal stent ends
relative to the lesion are still correct.
15. Rotate the wheel as shown in B of Figure 4 whilst holding the handle
in a fixed position to begin stent deployment under fluoroscopic
guidance. Stent deployment starts when the moving marker on
the retractable shaft passes the distal marker on the delivery
system as shown in Figure 5. Ensure proper stent positioning
before completely deploying and releasing the stent as this cannot
be done once the distal end of the stent is wall-apposed. DO NOT
constrict the retractable shaft or the blue stabilizer shaft with the
other hand that is holding the delivery system.
16. Continue turning the wheel and check for a steady gap between the
distal marker on the delivery system and the distal stent markers
as shown in Figure 6. The stent is fully deployed when the moving
marker on the retractable shaft passes the proximal marker
on the delivery system. If strong resistance is felt during stent
deployment, stop and determine the cause before proceeding.
17. Obtain angiographic visualization of the stented vessel segment.
Correct stent deployment (not compressed or stretched) can be
checked by matching the delivery system markers with the stent
markers.
Delivery System Removal
18. Remove the delivery system carefully under fluoroscopic guidance
after full stent deployment whilst observing the radiopaque marker
at the distal end and leaving the guide wire in place. If the tip does
not withdraw easily, determine the cause before reattempting
removal. The delivery system may be moved carefully in the distal
direction to free the tip.
19. Obtain angiographic visualization of the stented vessel segment.
If the stent is incompletely expanded along the lesion, a post
deployment balloon dilation (standard PTA) can be performed at
the discretion of the physician. Ensure that the inflated diameter
of the PTA balloon matches the reference diameter of the target
vessel.
20. After use, dispose the product and packaging in accordance with
hospital, administrative and/or local government policy.
MRI Safety Information
Non-clinical tests have demonstrated that the Pulsar-18 T3 stent
is MR conditional for single and overlapping lengths up to 385 mm.
A patient with this device can be safely scanned in an MR system
meeting the following conditions:
• Static magnetic field of 1.5 and 3.0 Tesla.
• Maximum spatial gradient magnetic field of 3000 gauss/cm
(30 T/m).
• Maximum MR system reported, whole-body-averaged specific
absorption rate (SAR) of 1 W/kg for landmarks below the umbilicus
and 2 W/kg (Normal Operating Mode) for landmarks above the
umbilicus.
Under the scan conditions defined above, the stent is expected to
produce a maximum temperature rise of 5.7 °C after 15 minutes of
continuous scanning.
In non-clinical tests, the stent caused the image artifact to extend
approximately 4 mm when imaged with a gradient echo sequence and
3 mm when imaged with a spin echo pulse sequence in a 3.0 Tesla MRI
system. The artifact may obscure the device lumen.
Warranty/Liability
This product and each of its components (hereinafter product) were
designed, manufactured, tested and packaged with all reasonable
care. However, since BIOTRONIK does not have control over the
conditions under which the product is used, the contents of this
Instructions For Use (IFU) are to be considered as an integral part of
this disclaimer for cases when a disturbance of the product’s intended
function may occur for various reasons.
BIOTRONIK does not guarantee that the following events will not
occur:
• Product malfunctions or failures
• Patient’s immune response to the product
• Medical complications during the use of the product or as a
consequence of the product being in contact with the patient’s body.
BIOTRONIK shall assume no liability for:
• The use of the product that is not in accordance with the stated
intended use/indication, contraindications, warnings, precautions
and the directions for use of this IFU
• Modification to the original product
• Causes which could not have been foreseen at the time of product
delivery using the available levels of science and technology
• Causes originating from other BIOTRONIK products or products
not from BIOTRONIK and force major events which include, but not
limited to, natural disasters.
The above provisions shall be without prejudice to any disclaimer and/
or limitation of liability agreed separately with the customer to the
extent permitted by applicable laws.
For US only:
BIOTRONIK disclaims all warranties, expressed or implied
regarding the product, including but not limited to, any warranty of
merchantability or fitness for a particular purpose of the product.
BIOTRONIK is not liable for any direct, incidental or consequential
damages or expenses caused by any use of the product whether the
claim is based on any theory of liability, including negligence.
Deutsch
Beschreibung
Das Stentsystem Pulsar-18 T3 (im Weiteren Pulsar-18 T3) wie in
Abbildung 1 gezeigt, ist ein selbstexpandierender Stent, der auf einem
drahtgeführten („Over-the-Wire“) Einführsystem vormontiert ist. Der
Stent (1) ist ein permanentes Implantat aus einem laser geschnittenen
Nitinolröhrchen. Der Stent (1) hat sechs Röntgen markierungen an
beiden Enden (1a, 1b) und ist vollständig mit einer dünnen Schicht
aus amorphem Siliziumkarbid (proBIO™) bedeckt.
Das Einführsystem besteht aus einer triaxialen Schaftkonstruktion:
der inneren Schafteinheit (2), dem mittleren zurückziehbaren Schaft
(3) und dem fixierten äußeren blauen Stabilisierungsschaft (11).
Das zentrale Führungsdrahtlumen in der inneren Schafteinheit (2)
beginnt an der Spitze (7) des distalen Einführsystems und endet
am Luer-Anschluss (6) am Griff (9). Die Spülung des Führungs-
drahtlumens erfolgt über den Luer-Anschluss (6).
Der Stent befindet sich zwischen der inneren Schafteinheit (2) und dem
zurückziehbaren Schaft (3) am distalen Ende des Einführsystems. Die
beiden Röntgenmarkierungen des Einführsystems (8a, 8b) erleichtern
Pulsar-18 T3_version A.indd 6
17.10.2018 14:21:57