













5-565.1
54
Job Name:
Date:
Address:
Model No.:
City & State:
Order No.:
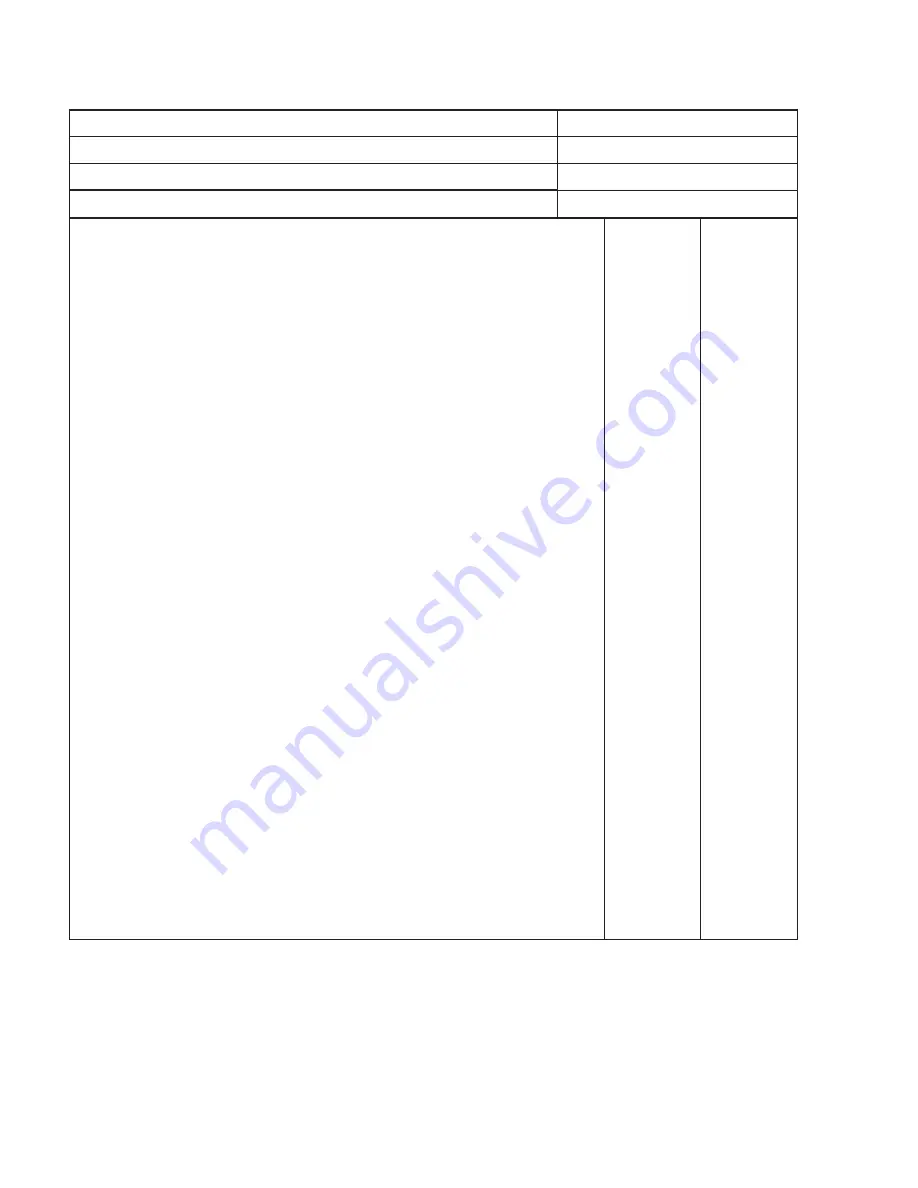
Start-Up Check List “ALL ITEMS MUST BE CHECKED”
Serial No.:
1. All shipping straps, braces, tie downs removed?
____ Yes
___ No
2. Unit installed level and secure?
____ Yes
___ No
3. Gas burner properly located and aligned?
____ Yes
___ No
4. Blower and motor alignment okay?
____ Yes
___ No
5. Bearings aligned and tight on shaft/bearing supports?
____ Yes
___ No
6. Electrical connections checked and secure?
____ Yes
___ No
7. Gas piping checked and tightened if necessary?
____ Yes
___ No
8. Any visible damage to unit?
____ Yes
___ No
Describe: ______________________________________________
If damaged, was the damage repaired?
____ Yes
___ No
9. Air inlet and discharge checked for obstructions?
____ Yes
___ No
10. Bearings checked for proper lubrication?
____ Yes
___ No
11. Filters in place and correct to direction of air flow?
____ Yes
___ No
12. Belt tension checked?
____ Yes
___ No
13. Electric supply to unit: ______ Volts, ______ Hz, ______ Phase
14. Gas supply to unit: ______ Natural, ______ Propane
15. Gas supply pressure to unit: ______ " W.C., ______ PSIG
16. Inlet and/or discharge dampers operating correctly?
____ Yes
___ No
17. Blower rotation correct?
____ Yes
___ No
18. Blower speed: Hi Speed ______ RPM, Lo Speed ______ RPM
19. Motor speed: Hi Speed ______ RPM, Lo Speed ______ RPM
20. Is unit noisy? Excessive vibration?
____ Yes
___ No
21. Motor voltage: L1 ______ V, L2 ______ V, L3 ______ V
22. Motor amps: L1 ______ Amp, L2 ______ Amp, L3 ______ Amp
23. High temperature limit control continuity checked?
____ Yes
___ No
24. Burner light off
Low Fire: Does entire burner light off?
____ Yes
___ No
Hi Fire: Burner pressure reading? ______ " W.C.
Is flame clean and stable?
____ Yes
___ No
Does flame modulate in response to temperature control(s)?
____ Yes
___ No
25. Gas input checked?
____ Yes
___ No
Input at maximum firing rate: __________ Btu/Hr
Input at minimum firing rate: -__________ Btu/Hr
26. Gas piping checked for and free of leaks?
____ Yes
___ No
27. Has wiring been verified to match the unit wiring diagram?
____ Yes
___ No
28. Have all the modes of the sequence of operation been verified and tested?
____ Yes
___ No
29. What optional and/or accessory control devices have been set?
Device: _______________ Setting: ___________ (°F/psi/Inches W.C./etc.) ____ Yes
___ No
Device: _______________ Setting: ___________ (°F/psi/Inches W.C./etc.) ____ Yes
___ No
Device: _______________ Setting: ___________ (°F/psi/Inches W.C./etc.) ____ Yes
___ No
indirect gas-fired Heating eQuiPment
Customer/Owner instructed in operation and maintenance of unit?
____ Yes
___ No
Name of Person(s) Instructed: ______________________________________________________________
Comments: ____________________________________________________________________________
____________________________________________________________________________
Start-Up Company Name: _______________________________ Phone: __________________________
Signature: _______________________________________________________ Date: ________________
start-uP cHecKlist






































































