

















Volaro Lift/Transfer Assessment Form
Are you using the correct lift for your needs?
Patient Name _________________________ ID#_________________Room#_____
Assessment Completed by____________________________Date_____________
Lift(s) Required___________________________Sling Size___________________
Comments for PRN Use_______________________________________________
Assessment Updated by_____________________________ Date_____________
_____________________________Date_____________
_____________________________Date_____________
Assessment Care Planned by_________________________Date_____________
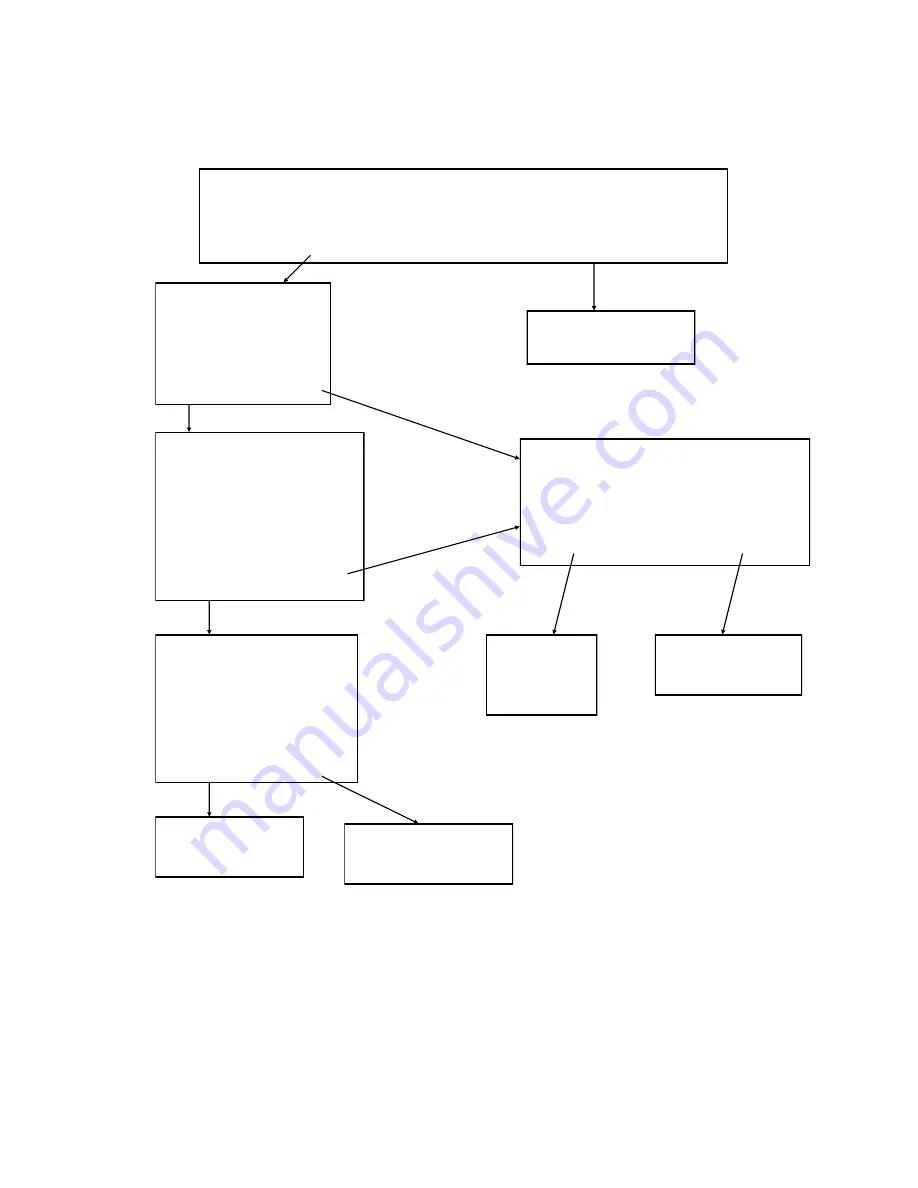
Can individual safely perform > or = 50% of lift / transfer
with only standby assistance from caregiver?
No
Yes
Can individual
bear weight on at
least one leg?
Yes
No
No Lift Needed.
Does the individual
have moderate upper
body strength and
ability to follow simple
commands?
Yes
No
Does the individual weigh less
than the maximum capacity of
the SMT Full Body Lift?
No
Yes
Does the individual
weigh less than the
capacity of the SMT
Sit
-
to
-
Stand Lift?
Yes
No
Sit
-
to
-
Stand
Recommended.
Contact Safety
Committee.
Contact
Safety
Committee.
Full Body Lift
Recommended.
3







































































