


















05
SPEX BACK SUPPORT USER MANUAL
16
WWW.SPEXSEATING.COM
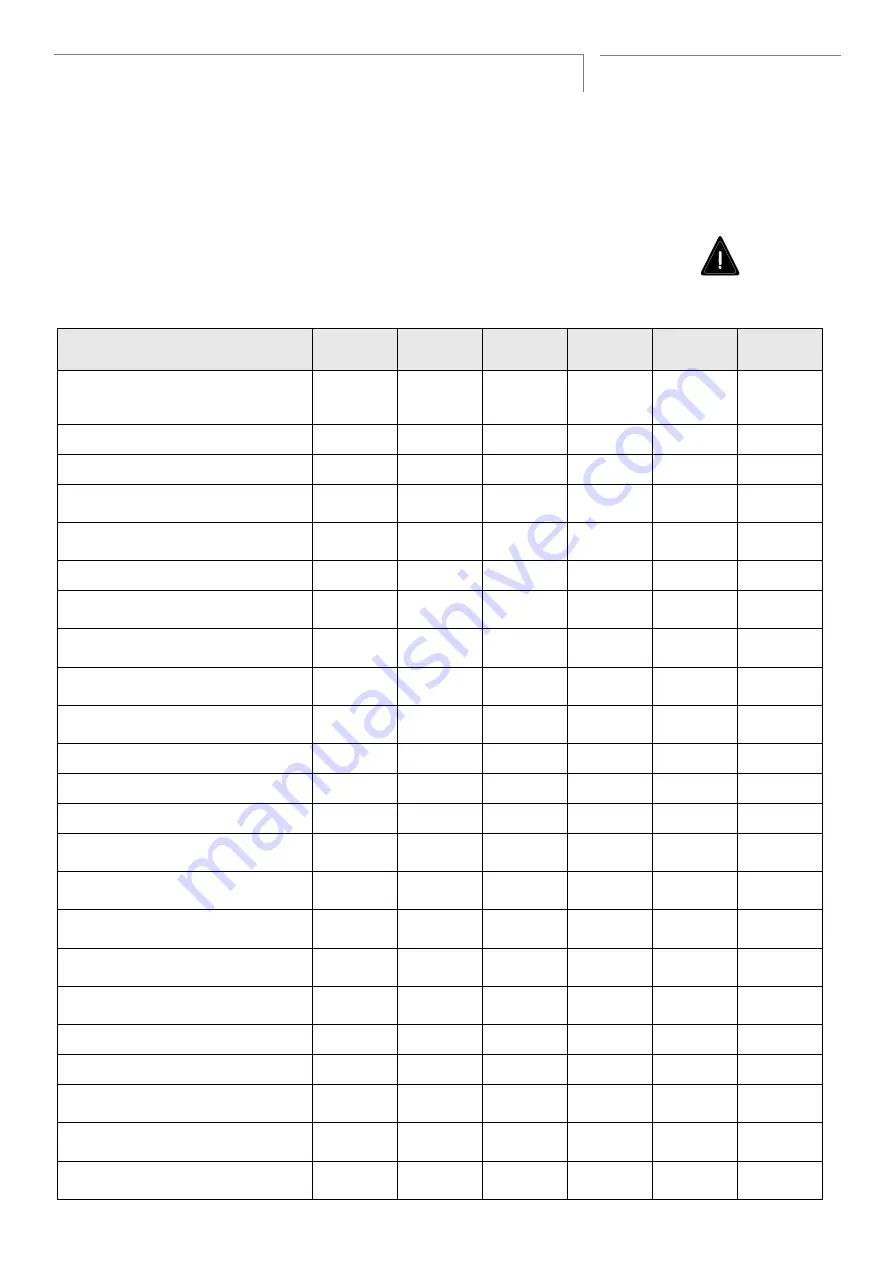
6 Month Checklist
Checklist
Date:
or
Date:
or
Date:
or
Date:
or
Date:
or
Date:
or
No concerns with the overall safety of the
user? If
, contact your therapist or Spex
distributor immediately.
No accidents occurred or harm caused?
No abnormal stress caused to the seating?
User is wearing an appropriate lap belt and
harness?
No bags or appendages present on the
seating which may cause stability issues?
User is under the maximum weight capacity?
Are the mounting clamps secured properly
to the wheelchair canes?
Are the quick release latches properly
engaging?
Are the nuts on the L-brackets and pins
secured?
Can the Back Support be removed &
installed properly?
Are all hardware and fasteners tight?
Are all components clean?
Are the covers clean and washed?
Is the cushion maintaining correct support
and control for the user’s pelvis?
Is the cushion adjusted correctly and not
modified adversely?
Is the cushion installed the right way on the
wheelchair?
Does the Back Support maintain correct
support and control?
Is the Back Support adjusted correctly and
not modified adversely?
Are the laterals adjusted correctly?
Is the headrest adjusted correctly?
Is a certified Wheelchair Tie-down & Occu-
pant Restraint System being correctly used?
Is set-up as per the Transit Safety section and
Warnings in this user manual?
Is the primary caregiver knowledgeable
about the above points?
The 6 month checklist is a compulsory check to ensure that your Back Support is
maintained in a safe and functional condition. The examiner must check each item
on the checklist and place the date and their initials in the appropriate column for
that check. Failure to perform these checks may void warranty.
Health & S
afet
y
Har
dw
ar
e
H
ygiene
User P
ostur
e
Tr
ansit
(if applic
able)







































































