














Your hearing aids
Hearing healthcare professional: _______________
__________________________________________
Telephone: _________________________________
Model: ____________________________________
Serial number: ______________________________
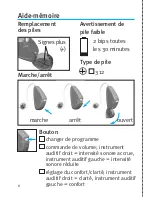
Replacement batteries:
Size 312
Warranty: __________________________________
Program 1 is the automatic program
Program 2 is for: ____________________________
Program 3 is for: ____________________________
Program 4 is for: ____________________________
Date of purchase: ___________________________
3







































































